
The pursuit of the athletes’ limits in sport to reach their maximum performance, can have as a consequence the risk of injury in this process. In men’s football, for example, there is an injury rate of 8 injures per 1000 hours of exposure.1 That is to say, a football player experiences an injure every 125 hours that they spend with the ball. A team of 25 players experiences an average of 50 injuries throughout a season, 12% of those are relapses. One out of four athletes from the United Kingdom Athletic team experienced an illness or an injury before, during or immediately after taking part in the 2012 Summer Olympics.2 The return-to-play decision (RTP) is complex and specific for each athlete and sport and it is frequently influenced by external factors (e.g. fan pressure, the media, a coach’s need to alter a losing streak or because a very important game or competition is coming up).3
There is an article advocating for the advantages of supporting shared decision-making between medical services, the athlete and the coach in order to choose the right moment to return to play. 4 The article, published in the British Journal of Sports Medicine in 2017, suggests three steps in this process:
- Choice: medical service professionals should inform the athlete and the coach about the reasonable options that exist.
- Option: providing more detailed information about the different options available.
- Decision: guiding the athlete and coach to decide what is best.
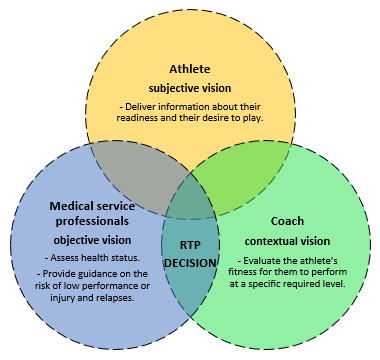
Those who take part in this shared decision-making process perform a key role in it (Figure 1). The medical service team are the most qualified to evaluate the athlete’s health status and provide an objective guidance to choose the moment to return to play after an injury. It is also recommended to be aware of the risks of low performance, relapses or injury in the short term, the consequences of a relapse and the long-term health risk that the athlete might face. This recommendation is mainly based on the clinical situation and the actual context of each athlete who has a specific problem. The professional experience, the type of injury, the individual relationship with the athlete, the demands of the competition and the published scientific evidence are key elements of the decision-making process. Athletes, when they are completely competent, should inform their readiness and their desire to play. This decision should be made considering the personal circumstances and experience, the persona perception of the possible risks, the environment, the specific information concerning their health and performance status. There are contextual factors at a high level that should also be considered, such as media pressure and sponsors. The coach assesses the athlete’s fitness to perform at a specific team and competition level, based on knowledge about the athlete, the training sessions they have missed, their functional progress during rehabilitation and the information provided by the medical service team. The contribution of the coach towards the shared decision-making process has to do with their knowledge about the specific sporting context. It is important to value the relevance of the player in the team, the importance of the game or competition coming up, the phase of the season, the availability of high-level substitutes and the risk that can be taken in the short, middle and long term for a relapse.
To sum up, medical services perform the key role of objectively informing athletes and coaches about the health status and the risk of injury or low performance. Athletes and coaches are the ones who will finally assess the information and make the decision about returning to play. Successful decision-making depends to a large extent on effective internal communication within the club staff teams.5
References:
1 Ekstrand J, Hägglund M, Waldén M. Injury incidence and injury patterns in professional football: the UEFA injury study. Br J Sports Med 2011; 45:553-558.
2 Dijkstra HP, Pollock N, Chakraverty R, et al. Managing the health of the elite athlete: a new integrated performance health management and coaching model. Br J Sports Med 2014; 48:523–31.
3 Creighton DW, Shrier I, Shultz R, et al. Return-to-play in sport: a decision-based model. Clin J Sport Med 2010; 20:379–85
4 Dijkstra HP, Pollock N, Chakraverty R, Ardem, Return to play in elite sport: a shared decision-making process Br J Sports Med 2017; 51:419-420.
5 Ekstrand J, Lundqvist D, Davison M, D´Hooghe, M, Pensgaard, A. Communication quality between the medical team and the head coach/manager is associated with injury burden and player availability in elite football clubs Br J Sports Med 2019; 53: 304-308
Carlos Lago Peñas
KNOW MORE
CATEGORY: MARKETING, COMMUNICATION AND MANAGEMENT
This model looks to the future with the requirements and demands of a new era of stadiums, directed toward improving and fulfilling the experiences of fans and spectators, remembering “feeling” and “passion” when designing their business model.
CATEGORY: FOOTBALL SPORTS PERFORMANCE
Through the use of computer vision we can identify some shortcomings in the body orientation of players in different game situations.
CATEGORY: MEDICINE HEALTH AND WELLNESS
A health check must detect situations which, despite not showing obvious symptoms, may endanger athletes subject to the highest demands.
CATEGORY: FOOTBALL TEAM SPORTS
In the words of Johan Cruyff, “Players, in reality, have the ball for 3 minutes, on average. So, the most important thing is: what do you do during those 87 minutes when you do not have the ball? That is what determines whether you’re a good player or not.”
CATEGORY: MEDICINE HEALTH AND WELLNESS SPORTS PERFORMANCE
Muscle injuries account for more than 30% of all injuries in sports like soccer. Their significance is therefore enormous in terms of training sessions and lost game time.
DO YOU WANT TO KNOW MORE?
- SUBSCRIBE
- CONTACT
- APPLY
KEEP UP TO DATE WITH OUR NEWS
Do you have any questions about Barça Universitas?
- Startup
- Research Center
- Corporate